Beyond weight loss: can Ozempic and its relatives protect the brain?
A wave of clinical trials has tested whether GLP-1 receptor agonists — the blockbuster diabetes and weight-loss drugs — can slow Alzheimer’s, Parkinson’s, and other neurodegenerative diseases. The results have been sobering, occasionally promising, and scientifically revealing.
It is one of the most audacious hypotheses in modern neurology: that a drug designed to mimic a gut hormone could slow the destruction of the human brain. On its face, the idea seems improbable — what business does a digestive signal have protecting neurons from amyloid plaques, tau tangles, or alpha-synuclein aggregates?
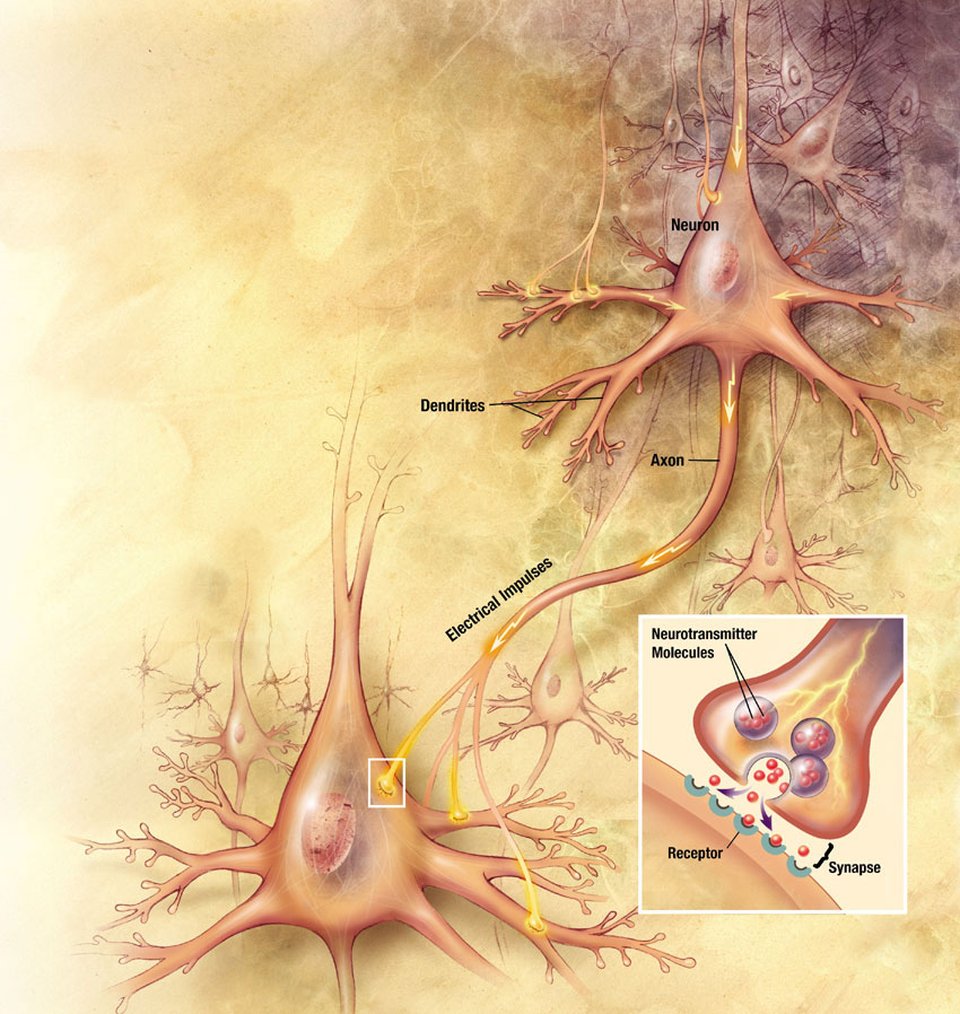
But GLP-1 receptors are not confined to the pancreas. They are expressed throughout the brain — in the hippocampus, the substantia nigra, the cortex, the amygdala, and the hypothalamus. Endogenous GLP-1 is produced by neurons in the nucleus tractus solitarius and projects widely through subcortical pathways. When researchers began to notice, in the early 2010s, that GLP-1 receptor agonists could reduce neuroinflammation, oxidative stress, and apoptosis in animal models, a new line of inquiry was born.
More than a decade later, the clinical picture has emerged. And it is far more complicated than the headlines have suggested.
The molecular case: why the brain might listen
To understand why GLP-1 drugs were ever considered for neurodegenerative disease, one needs to look inside the neuron.
GLP-1 receptors are G-protein-coupled receptors. When activated, they trigger a cascade of intracellular signals — primarily through the cAMP/PKA pathway, the PI3K/Akt survival pathway, and the MAPK/ERK cascade. These pathways converge on the transcription factor CREB, which upregulates brain-derived neurotrophic factor (BDNF) — a protein essential for synaptic plasticity and neuronal resilience.
In preclinical models, GLP-1 receptor agonists have been shown to:
- Suppress neuroinflammation — by inhibiting NF-κB signalling, shifting microglia from the pro-inflammatory M1 phenotype toward the anti-inflammatory M2 state, and reducing NLRP3 inflammasome activation, lowering IL-1β and TNF-α.
- Reduce oxidative stress — by activating the transcription factor Nrf2, which upregulates antioxidant enzymes including superoxide dismutase, catalase, glutathione peroxidase, and haem oxygenase-1.
- Protect mitochondria — through PGC-1α activation, which promotes mitochondrial biogenesis, and enhanced PINK1/Parkin-dependent mitophagy.
- Inhibit neuronal apoptosis — via PI3K/Akt-mediated suppression of Bad, Bax, and caspase-9, and phosphorylation (inhibition) of GSK-3β.
- Ameliorate amyloid pathology — through increased clearance of amyloid-beta and reduced tau hyperphosphorylation, mediated in part by autophagy enhancement.
The evidence is strongest in animal models. Liraglutide, exenatide, and semaglutide have each shown protection against amyloid-beta toxicity, MPTP-induced dopaminergic neuron loss, and cognitive decline in transgenic mice. The pioneer of this line of research, Christian Hölscher (formerly of Lancaster University), has argued since 2012 that GLP-1 acts as a CNS growth factor — a “pharmacological analogue of exercise,” as he put it in a 2025 review in CNS Drugs.
But mechanism is not outcome. The gap between a well-tuned molecular pathway and a clinically meaningful result in a human patient is precisely what the next decade of trials set out to measure — and largely failed to cross.
Alzheimer’s disease: the EVOKE disappointment
The highest-stakes test of the GLP-1 neuroprotection hypothesis was the EVOKE and EVOKE+ program — two identically designed Phase III trials sponsored by Novo Nordisk, testing oral semaglutide (14 mg once daily) in 3,808 adults with early Alzheimer’s disease (mild cognitive impairment or mild dementia, amyloid-confirmed).
The trials were massive — run across 566 sites in 40 countries, with a 104-week main treatment phase and a planned 52-week extension. The primary endpoint was the change in CDR-SB (Clinical Dementia Rating — Sum of Boxes), a standard scale that measures both cognitive and functional decline.
On November 24, 2025, Novo Nordisk announced top-line results: both trials failed to meet their primary endpoint. The extension was discontinued. Full results were published in The Lancet on March 19, 2026, presented simultaneously at the AD/PD 2026 conference.
The numbers tell a stark story:
| Measure | EVOKE | EVOKE+ |
|---|---|---|
| CDR-SB difference vs. placebo | −0.06 points (favors drug, p=0.77) | +0.15 points (favors placebo, p=0.46) |
| ADCS-ADL-MCI (daily function) | No significant difference | No significant difference |
| Time to dementia progression | No difference | No difference |
| Subgroup analysis (age, sex, BMI, T2D) | No signal in any subgroup | No signal in any subgroup |
The biomarker picture was more interesting — but ultimately unhelpful. In a CSF sub-study of ~210 participants, semaglutide produced modest reductions in p-tau181 (~10%), YKL-40 (a neuroinflammation marker, ~10%), and neurogranin (a synaptic marker, ~10%). Plasma high-sensitivity CRP — a marker of peripheral inflammation — dropped significantly by 24–29%, confirming the drug’s well-known systemic anti-inflammatory effect.
But cognition did not follow. As Jeffrey Cummings (University of Nevada, Las Vegas), who presented the data at CTAD 2025, put it: “Our underlying hypothesis was that, if we could suppress peripheral inflammation, we will have a beneficial impact on cognition. We did significantly suppress peripheral inflammation. We did not have the corresponding benefit on cognition.”
The liraglutide signal that preceded it
The EVOKE failure makes an earlier trial all the more tantalizing — and puzzling. The ELAD trial, a Phase IIb study of liraglutide (1.8 mg subcutaneous daily) in 204 patients with mild-to-moderate Alzheimer’s, missed its primary endpoint (change in cerebral glucose metabolism on PET). But secondary and exploratory analyses, published in Nature Medicine in December 2025, found that liraglutide was associated with 18% slower cognitive decline and ~50% less brain volume loss in frontal, temporal, parietal, and total grey matter.
Why would liraglutide show signals that semaglutide — a more potent, longer-acting molecule — could not replicate? Several hypotheses are being actively debated:
- Blood-brain barrier penetration. Liraglutide and semaglutide are large peptides with limited CNS access; both act primarily through circumventricular organs and areas where the blood-brain barrier is leaky. But subtle differences in molecular structure may affect how much drug reaches brain parenchyma.
- Patient population. ELAD enrolled mild-to-moderate Alzheimer’s without requiring amyloid confirmation. EVOKE required amyloid positivity. The former may have included patients with mixed pathology (vascular + neurodegenerative) who respond differently.
- Disease stage. By the time patients have amyloid-confirmed cognitive impairment, neurodegenerative damage may be too advanced for GLP-1 mechanisms — which are primarily anti-inflammatory and metabolic — to alter the trajectory.
- Statistical noise. The ELAD’s positive secondary findings may simply be false positives. The study was small (204 patients), and the pre-specified primary endpoint was negative.
Parkinson’s disease: a paradox of positive trials and a failed Phase III
The Parkinson’s story follows a similar arc — with an additional twist.
GLP-1 receptors are densely expressed in the substantia nigra, where dopaminergic neurons are progressively lost in Parkinson’s disease. Michael J. Fox Foundation and Cure Parkinson’s have both invested heavily in GLP-1 repurposing trials. The preclinical rationale is strong: GLP-1 agonists protect dopaminergic neurons from MPTP and 6-OHDA toxicity in rodents, reduce alpha-synuclein aggregation, and improve motor function.
Three earlier trials had suggested benefit:
| Trial | Drug | n | Duration | Result |
|---|---|---|---|---|
| Aviles-Olmos (2013) | Exenatide | 45 | 12 months | +4.9 point MDS-UPDRS benefit (p=0.037) |
| Athauda / Exenatide-PD2 (2017, Lancet) | Exenatide 2 mg weekly | 62 | 48 weeks + 12 washout | 3.5-point benefit (p=0.032); persisted after washout |
| Meissner / LIXIPARK (2024, NEJM) | Lixisenatide 20 mcg daily | 156 | 12 months | 3.08-point benefit (p=0.007); effect held after washout |
The LIXIPARK result was perhaps the most encouraging. In early Parkinson’s (≤3 years since diagnosis), the placebo group worsened by 3.04 points on the MDS-UPDRS Part III (motor score) over 12 months; the lixisenatide group stayed essentially flat (−0.04 points). The 3.08-point difference was statistically significant (p=0.007), and the effect persisted during a 2-month washout period — hinting at disease modification rather than mere symptom relief. Wassilios G. Meissner (University Hospital Bordeaux) and Olivier Rascol (University Hospital Toulouse) led the trial, published in the New England Journal of Medicine in April 2024.
Then came Exenatide-PD3.
The Phase III trial, led by Tom Foltynie (UCL Queen Square Institute of Neurology), enrolled 194 patients with moderate Parkinson’s and gave them weekly exenatide or placebo for 96 weeks — twice the duration of the positive Phase IIb. The result, published in The Lancet in February 2025: no significant difference between groups. The exenatide group worsened by 5.7 points; the placebo group by 4.6 points. All secondary endpoints were also negative.
Per Parkinson’s UK and the Michael J. Fox Foundation, the trial did not support exenatide as a disease-modifying treatment for Parkinson’s.
Why the discrepancy?
Several explanations are being explored:
- Disease stage. LIXIPARK enrolled patients within 3 years of diagnosis. Exenatide-PD3 enrolled patients with ~6 years since diagnosis. By the time moderate disease is established, the window for GLP-1 intervention may have closed.
- Drug differences. Lixisenatide and exenatide are not identical. Lixisenatide has been reported to cross the blood-brain barrier more effectively than exenatide, and their receptor binding profiles differ.
- Dose and duration. It is possible that 96 weeks is insufficient to detect a disease-modifying effect — or, conversely, that any benefit of GLP-1 agonism wanes over time as the underlying pathology progresses beyond the reach of anti-inflammatory mechanisms.
Ongoing trials may resolve some of these questions. The GIPD study (semaglutide 1.0 mg weekly, 270 patients, Oslo University Hospital) and the MOST-ABLE study (oral semaglutide, Japan) are both testing GLP-1 agonists in earlier-stage Parkinson’s. Results are expected in 2026–2027.
Epidemiological clues
While clinical trials in established disease have delivered mostly negative results, a parallel line of evidence has emerged from observational studies of people with type 2 diabetes — the population already taking GLP-1 drugs for metabolic reasons.
These studies consistently find that diabetes patients prescribed GLP-1 receptor agonists have a 40–70% lower risk of being diagnosed with dementia or Alzheimer’s disease compared with patients on other diabetes medications.
| Study | Population | Finding |
|---|---|---|
| Wang et al. (2024, Alzheimer’s & Dementia) | 1,094,761 US patients with T2D | Semaglutide associated with 40–70% lower Alzheimer’s risk vs. other diabetes drugs |
| Lin et al. (2025, JAMA Network Open) | T2D + obesity | Dementia hazard ratio 0.63 (95% CI 0.50–0.81) |
| Tang et al. (2025, JAMA Neurology) | T2D patients | Alzheimer’s-related dementia HR 0.67 (95% CI 0.47–0.96) |
| Brauer et al. (2020, Brain) | 100,288 UK T2D patients | 62% reduced Parkinson’s incidence (IRR 0.38, 95% CI 0.17–0.60) |
A 2025 meta-analysis in JAMA Neurology of 26 randomized trials found GLP-1 receptor agonists associated with lower odds of dementia overall (odds ratio 0.55, 95% CI 0.35–0.86).
These numbers are striking — and they are also difficult to interpret. As Eric Widera (UCSF) pointed out in a 2025 commentary in Alzheimer’s & Dementia, some studies showed reduced Alzheimer’s risk within 30 days of a first prescription. That is biologically implausible for a genuine disease-prevention effect. It suggests that healthy-user bias — patients who receive newer, more expensive drugs tend to be more engaged with healthcare and lead healthier lives — or survival bias (GLP-1 drugs reduce cardiovascular death, giving patients more time without an Alzheimer’s diagnosis) are at play.
Still, the signal is large, consistent across multiple independent cohorts, and not explained away by any single confounder. The best interpretation may be that GLP-1 drugs reduce dementia risk in people with diabetes through indirect mechanisms — improved glycemic control, reduced cardiovascular events, lower blood pressure, weight loss — rather than through direct neuroprotection.
What comes next
The clinical trial record so far can be summarized bluntly: GLP-1 receptor agonists do not appear to slow established Alzheimer’s or Parkinson’s disease, at least not with the molecules and trial designs tested to date.
But the field is far from abandoning the hypothesis. Several directions remain open:
Prevention trials
The large observational signals in diabetes populations — combined with the failure of EVOKE in symptomatic Alzheimer’s — have shifted attention toward primary prevention: testing GLP-1 drugs in cognitively healthy people at risk for dementia, before significant neurodegeneration has occurred. No such trial is yet underway, but the case is being made.
Dual and triple agonists
The commercial landscape of incretin drugs is evolving rapidly. Tirzepatide (Mounjaro/Zepbound) is a dual GLP-1/GIP receptor agonist; retatrutide is a triple GLP-1/GIP/glucagon agonist. These molecules are more potent metabolically and may have different CNS profiles.
Preclinically, the GLP-1/GIP dual agonist DA5-CH, developed by Christian Hölscher’s group, has shown neuroprotective effects superior to single-receptor agonists in both Alzheimer’s and Parkinson’s rodent models — including in a new study published in Frontiers in Endocrinology (2026) showing superiority to both tirzepatide and exenatide in the 6-OHDA rat model of Parkinson’s. Whether this translates to humans remains unknown.
Better blood-brain barrier penetrators
Most current GLP-1 drugs are large peptides with limited CNS access. Next-generation molecules designed specifically for brain penetration — smaller molecules, or those using transporter-mediated delivery — could produce higher target engagement in the CNS. Novo Nordisk’s oral semaglutide (Rybelsus) is already a step in this direction, but the EVOKE results suggest it was not enough.
The metabolic link
There is growing evidence that insulin resistance and metabolic dysfunction are early contributors to neurodegeneration — sometimes called “type 3 diabetes.” GLP-1 agonists improve cerebral insulin signalling. If this is the relevant mechanism, then the drug may need to be given early — before synaptic damage is irreversible — and for long durations.
The sober bottom line
For a patient with Alzheimer’s or Parkinson’s today, a GLP-1 receptor agonist is not a proven disease-modifying therapy. No regulatory body has approved one for either indication, and the largest, most rigorous trials have delivered negative results.
But the story is not over. The CSF biomarker reductions in EVOKE suggest semaglutide is doing something in the brain — just not enough to change clinical trajectory in patients who are already symptomatic. The epidemiological signals in diabetes populations are too large and consistent to dismiss. The liraglutide-associated brain volume preservation seen in ELAD, if real, would be a finding of enormous importance.
The most honest summary, as of May 2026, may be this: the brain pays attention to GLP-1. It just does not yet listen well enough to make a difference — at least not with the tools we have tried, in the patients we have tested, on the timelines we have measured.
Future trials will need to be preventive, will need to use more brain-penetrant molecules, and may need to target patients with metabolic dysfunction long before their first cognitive symptom appears. That is a harder ask than simply repurposing a blockbuster drug. But it is also a more intellectually honest one.
Sources: Cummings J, et al. The Lancet (2026); Edison P, et al. Nature Medicine (2025); Vijiaratnam N, et al. The Lancet (2025); Meissner WG, et al. NEJM (2024); Hölscher C. CNS Drugs (2025); Brauer R, et al. Brain (2020); Wang W, et al. Alzheimer’s & Dementia (2024); Lin et al. JAMA Network Open (2025); Tang et al. JAMA Neurology (2025)