Published: June 03, 2026, 02:02 UTC
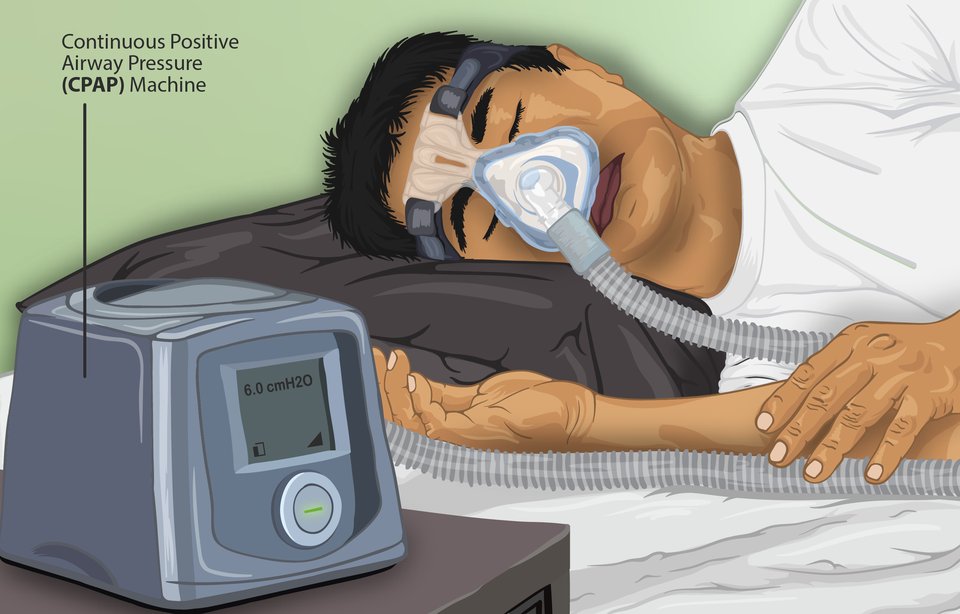
For the nearly one billion people worldwide living with obstructive sleep apnea (OSA), the standard of care — a Continuous Positive Airway Pressure (CPAP) machine — comes with an unglamorous reality: roughly half of patients abandon the device within a year. The mask is uncomfortable, the machine is noisy, and sleeping tethered to a bedside pump is, for many, simply unsustainable.
But a pharmacological alternative may finally be on the horizon. Two parallel Phase 3 clinical trials have demonstrated that a once-nightly oral pill called AD109 can reduce sleep apnea severity by roughly 44%, offering the first credible drug-based alternative to mechanical airway splinting. The results were published simultaneously in the American Journal of Respiratory and Critical Care Medicine (AJRCCM) and presented at the American Thoracic Society (ATS) 2026 International Conference in Orlando on May 17–19.
The Problem with CPAP
Obstructive sleep apnea occurs when the muscles of the upper airway — particularly the genioglossus, the tongue’s primary protrusor — relax too much during sleep, causing the pharynx to collapse repeatedly through the night. Each collapse stops breathing for 10 seconds or longer, starves the blood of oxygen, and triggers a micro-arousal that fragments sleep architecture. The result is a cascade of consequences: daytime sleepiness, cognitive impairment, hypertension, increased cardiovascular risk, and metabolic dysfunction.
CPAP works by physically stenting the airway open with positive air pressure via a mask. When used consistently, it is extraordinarily effective — capable of reducing the Apnea-Hypopnea Index (AHI, the number of breathing interruptions per hour of sleep) by 90% or more. But the compliance statistics tell a stark story: 30–50% of patients stop using it within the first year, and long-term adherence hovers around 40–60%.
How AD109 Works
AD109, developed by Cambridge, Massachusetts-based Apnimed, Inc., takes an entirely different approach. Rather than mechanically propping the airway open, it targets the root neuromuscular cause of OSA at the level of the brainstem.
During sleep, the hypoglossal motor nucleus — the cluster of neurons that controls tongue and upper airway muscles — loses its normal balance of inputs. Excitatory norepinephrine signaling declines, while inhibitory muscarinic acetylcholine signaling increases. The net effect is that the genioglossus relaxes and the airway narrows or collapses.
AD109 is a fixed-dose combination of two established drugs:
- Atomoxetine (75 mg) — a selective norepinephrine reuptake inhibitor that restores excitatory drive to the hypoglossal motor nucleus.
- Aroxybutynin (2.5 mg) — a novel antimuscarinic that blocks muscarinic acetylcholine receptors, reducing the inhibitory signal.
Together, they rebalance the neuromuscular control of the upper airway, effectively “keeping the throat awake” during sleep without waking the person. The approach is sometimes described as a neuromuscular modulator — a pharmacological alternative to the electrical hypoglossal nerve stimulators (like Inspire) that have emerged as second-line therapy for CPAP failure.
The Data: SynAIRgy and LunAIRo
SynAIRgy (NCT05813275) enrolled 646 adults with mild-to-severe OSA who had either failed or refused CPAP therapy, across 73 centers in the US and Canada. The primary endpoint was the change in AHI from baseline to week 26.
The results, published in AJRCCM by lead investigator Patrick John Strollo, MD (University of Pittsburgh/VA Pittsburgh Healthcare System), showed:
- Intent-to-treat analysis: AD109 reduced AHI by approximately 44% from baseline, compared to 18% with placebo (p = 0.001).
- On-treatment analysis (patients adhering to the drug): A 55.6% reduction in AHI versus 19.1% with placebo (p < 0.0001).
- 39.6% of participants achieved a ≥50% reduction in AHI.
- 22.3% achieved disease control, defined as AHI < 5 events per hour — essentially a cure.
- Significant improvements were also seen in oxygen desaturation index (ODI), hypoxic burden, and self-reported snoring.
LunAIRo (NCT05811247), the confirmatory Phase 3 trial, enrolled 660 adults across 64 US centers with an identical 26-week design. It met its primary endpoint with a 46.8% AHI reduction from baseline (p < 0.001). No serious treatment-related adverse events were reported in either trial.
A pooled analysis of both trials, presented at ATS 2026, confirmed a model-estimated AHI reduction of 39.3% with AD109 versus 12.6% with placebo.
Safety and Tolerability
The efficacy comes with a trade-off: 70.8% of AD109 recipients reported at least one adverse event, compared to 46.7% with placebo. The most common side effects — dry mouth, insomnia, nausea, urinary hesitation, constipation, and somnolence — are consistent with the known pharmacology of the two components (anticholinergic effects from aroxybutynin, sympathetic activation from atomoxetine).
21.2% of participants discontinued AD109 due to side effects, compared to just 3.1% on placebo — a tolerability signal that will be important for real-world use. No serious treatment-related adverse events were reported.
Regulatory Path
The FDA granted AD109 Fast Track designation in June 2022. Apnimed submitted a New Drug Application (NDA) to the FDA in early 2026. With the ATS data now published and the NDA under review, the PDUFA target action date — the FDA’s deadline for a decision — falls in Q1 2027.
Apnimed has secured $150 million in debt financing from HealthCare Royalty Partners to support a potential commercial launch, suggesting the company is preparing for a positive FDA decision.
The Caveats
The headline numbers are promising but deserve context. A ~44% AHI reduction is clinically meaningful, but it falls well short of what CPAP can achieve (~90+% reduction in adherent users). More than 60% of patients in the trials did not achieve a 50% reduction in AHI. And the 21% discontinuation rate due to side effects means tolerability will limit the drug’s addressable population.
The trials also enrolled patients who had already failed or refused CPAP — a “salvage” population. How AD109 performs in CPAP-naive patients, or head-to-head against CPAP, remains unknown. Long-term cardiovascular safety — particularly relevant given atomoxetine’s noradrenergic mechanism — has not been established beyond the 26–51 week trial windows.
What’s Next
If approved, AD109 would fill a specific niche: the millions of patients with mild-to-moderate OSA who cannot tolerate CPAP and either refuse or are ineligible for surgical options like hypoglossal nerve stimulation. It is unlikely to replace CPAP for severe disease, but it could meaningfully expand the therapeutic toolkit.
And it opens a new pharmacological axis for sleep medicine. If neuromuscular modulation works for sleep apnea, the same approach might eventually be refined — different drug combinations, different receptor targets — to improve efficacy and reduce side effects. The era of “a pill for sleep apnea” may finally be arriving, albeit with realistic expectations.
Source: Strollo PJ, et al. SynAIRgy Investigators. AD109, a Fixed-Dose Combination of Aroxybutynin and Atomoxetine, for the Treatment of Obstructive Sleep Apnea: Results From Two Phase 3 Trials. Am J Respir Crit Care Med. Published online May 18, 2026. DOI: 10.1164/rccm.202601-0083OC. ClinicalTrials.gov identifiers: NCT05813275 (SynAIRgy), NCT05811247 (LunAIRo). Apnimed, Inc. ATS 2026 International Conference, Orlando, FL, May 17–19, 2026.