A postmortem study published in the Journal of Sleep Research reports an almost complete loss of corticotropin-releasing hormone (CRH) neurons in the hypothalamic paraventricular nucleus of a woman who lived with narcolepsy without cataplexy for nearly three decades. The finding adds weight to the emerging idea that CRH neuron pathology contributes to excessive daytime sleepiness independently of the hypocretin system, and it raises new questions about how narcolepsy subtypes are defined.
What the Study Shows
Researchers at the Netherlands Institute for Neuroscience and French national sleep centers examined brain tissue from a 42-year-old woman who had experienced excessive daytime sleepiness since age 15. She never developed cataplexy and had no family history of narcolepsy. Her symptoms included frequent refreshing naps, hypnagogic hallucinations, and recurrent sleep paralysis. Her Epworth Sleepiness Scale score was 21, indicating severe sleepiness.
Clinically, her case was ambiguous. Cerebrospinal fluid hypocretin-1 was measured at 100 pg/mL in 2004 and 122 pg/mL in 2012, placing it in the borderline low-intermediate range (the diagnostic cutoff for narcolepsy type 1 is 110 pg/mL). She was HLA DQB1*06:02 positive, a strong genetic risk marker. Multiple Sleep Latency Tests performed eight years apart showed mean sleep latencies of 8.3 minutes (with three sleep-onset REM periods) and 10.8 minutes (with two SOREMPs) results that fall short of the classic narcolepsy diagnostic thresholds.
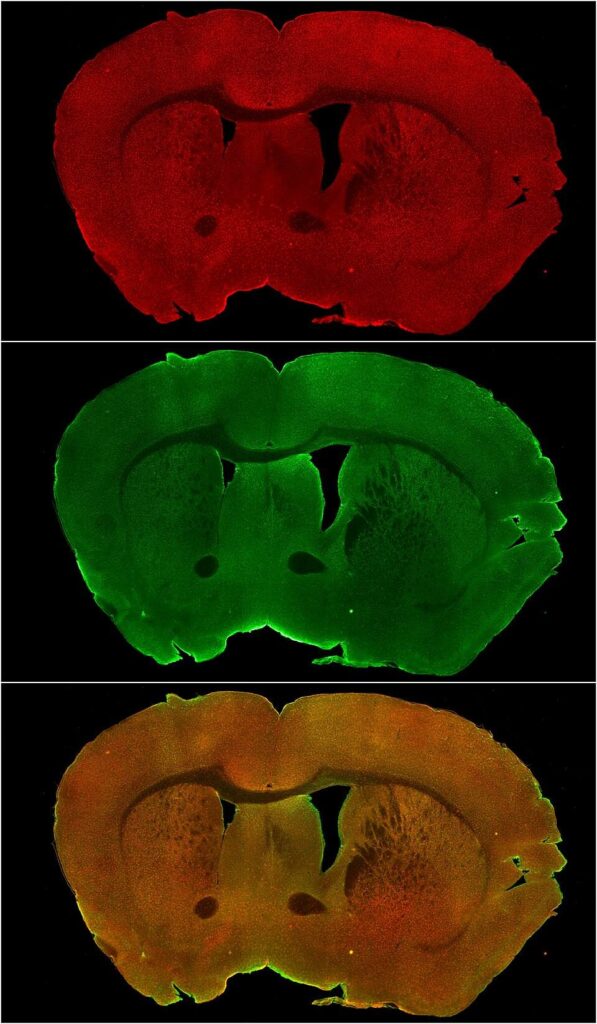
Postmortem analysis revealed something striking. Immunohistochemical staining of the paraventricular nucleus showed an almost complete loss of CRH-producing neurons, a pattern indistinguishable from a previously reported narcolepsy type 1 case. Unfortunately, the hypocretin-producing region of the hypothalamus was missing from the tissue block, so the researchers could not directly quantify hypocretin neuron loss. Nonetheless, the CRH finding stands on its own.
Why It Matters
This is the first report of marked CRH neuron reduction in a person with narcolepsy without cataplexy and borderline hypocretin levels. The finding is notable because CRH neurons in the paraventricular nucleus are best known for orchestrating the stress response via the hypothalamic-pituitary-adrenal axis. Their loss in narcolepsy suggests a broader hypothalamic pathology than previously recognized, one that may independently drive sleepiness.
The case also underscores a persistent diagnostic challenge. Current narcolepsy classification relies heavily on cataplexy and clear hypocretin deficiency, but this patient fell between categories. Her symptoms were real and severe, yet she did not fully meet criteria for either type 1 or type 2 narcolepsy. The postmortem finding of CRH loss, similar to what is seen in type 1, hints that the biology of narcolepsy may span a wider spectrum than current labels capture.
As with any single case report, caution is warranted. One patient cannot define a disease mechanism, and the missing hypothalamic tissue means we cannot rule out concurrent hypocretin loss. But postmortem human brain tissue from well-characterized narcolepsy patients is exceedingly rare, and every such case provides data that no animal model or imaging study can replicate. These findings point toward CRH neurons as a potentially overlooked player in the neurobiology of excessive daytime sleepiness, and they invite larger, confirmatory studies.
Source: Shan L, Linssen S, Fronczek R, Barateau L, Peyron C, Dauvilliers Y. Postmortem evidence of CRH neuron reduction in narcolepsy without cataplexy with borderline hypocretin-1 levels. Journal of Sleep Research. 2026 Jun 25. doi: 10.1111/jsr.70395. Open access.